Cannabis and Aspergillus: Exploring Medical Case Studies
I’m going to start this by stating that I am not a doctor, and the reason that I have linked all of the studies that I’m using is so that…
I’m going to start this by stating that I am not a doctor, and the reason that I have linked all of the studies that I’m using is so that people can find and read these articles for themselves — ultimately I am writing this series of articles as an informative resource for anyone wanting to understand more about the intersection of Aspergillus and cannabis. I will try my best to de-jargonify the findings of the scientific resources linked.
This is the second in a series of articles I’m writing about the intersection of Aspergillus and cannabis. The articles are:
- A Brief History of Aspergillus.
- Cannabis and Aspergillus: Exploring the Medical Literature (This Article).
- How is Cannabis tested for Aspergillus, and how are those tests regulated by the individual states?
- What’s a Farm to Do? Information on Methods of Prevention and Remediation of Aspergillus
- Case Study: An Organic Oregon Farm Engaging in Aspergillus Prevention
I will update the above links as the articles become available.
One of the reasons I wanted to create this article is that I wanted to make a space to honor these patients and their experiences. I also feel it’s important to fully explore these experiences to understand the medical risks that happen with aspergillus, specifically as it applies to cannabis.
I have a touch of medical data expertise — I co-authored a paper on synthesizing pediatric EHR data across six hospitals, and had a 20 year career in health analytics — but I am not a doctor. What I do have is a talent for translating difficult to understand medical information into business-speak and technical-speak. My intent is to make this information more accessible so that people can understand what the literature says, and will know where to look if they want more information.
AGAIN — I am not a doctor, I don’t even play one on TV! Don’t look at me as an expert — instead, let’s learn together!
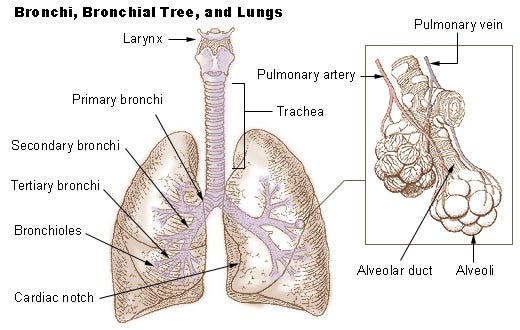
First, let’s take a quick look at this lung diagram and get to know the structures of the lung — it’ll come in handy as we figure out what happened to these patients.
Aspergillus and its General Health Impacts
A lot of the discourse that I’ve heard in the cannabis industry about Aspergillus is around the specific intersection between Aspergillus and cannabis, but I wanted to spend some time discussing what the medical impacts of Aspergillus are, before we get into the specifics with cannabis. I extensively cover the cases where Aspergillus intersects with cannabis, I will not be doing the same exhaustive coverage of Aspergillus in general, but you can read more about that here and in the Further Reading / Watching section of this article.
As we talked about in the first article, the first documented case of Aspergillosis was in 1789 when Jacques Thibault, a young soldier, presented at Paris Hospital with a protruding right eye and elevated cheekbone. Physicians found a fungal mass that they couldn’t simply cut due to the patient’s excessive bleeding. Eventually through several surgeries and cauterization (which at the time was done via branding irons — ouch!) Jacques’ case was cured, and he was released from the hospital over 100 days later.
Since then, our understanding of Aspergillosis — and Aspergillus species — has grown. While several years ago it was ‘common knowledge’ that Aspergillus fumigatus (A. fumigatus) was ‘the cause of 90% of infections’ it’s recently been written that species prevalence has changed over the last decade, and A. fumigatus is now responsible for around 60% of infections, followed by Aspergillus flavus, Aspergillus niger, and Aspergillus terreus. The World Health Organization (WHO) recently added Aspergillus to their watch list.
While invasive pulmonary aspergillosis (IPA) is associated with the immunocompromised and the immunosupressed, it doesn’t represent the whole of medical impacts of Aspergillus. Exposure to Aspergillus can also cause Allergic Bronchopulmonary Aspergillosis (ABPA), Aspergillus Bronchitis, Aspergillus Sinusitis, Chronic Pulmonary Aspergillosis (CPA) and Aspergilloma, Severe Asthma with Fungal Sensitisation (SAFS), Primary Cutaneous (skin) aspergillosis (PCA), and Aspergillus Endophthalmitis (aspergillus-related infections of the eye).
Aspergillus Bronchitis
A chronic illness where aspergillus causes an infection in the bronchi. Patients with cystic fibrosis, bronchiectasis (a condition that causes the thickening of the walls of the bronchi), and who are immunocompromised have higher risk. Aspergillus bronchitis is used to describe people with chronic pulmonary symptoms, but who don’t meet all the diagnostic categories. It can also cause bronchiectasis. This is another poorly understood diagnosis, and recent reviews of literature have found instances of Aspergillus Bronchitis in the immunocompetent. Treatment is itraconazole or voriconazole for four months, but relapse on discontinuation of the medications is common.
The symptoms include symptoms of a lower airway disease for over one month, positive sputum sample, slightly weakened immune system, high immunoglobulin G (IgG) levels, fungus growing in airways, or plugs of mucus seen with a bronchoscopy, and that it responds to antifungal medication after eight weeks of treatment.
Aspergillus sinusitis
This is when aspergillus-caused disease happens within the sinus — and this condition can lead to invasive pulmonary aspergillosis. Allergic fungal rhinosinusitis has the symptoms of a blocked-up or runny nose, and can lead to nasal polyps. In 1979, 79 cases had been identified in the prior decade, 42 of which were attributed to A. fumigatus. A couple of decades later, an increase of cases was acknowledged in the medical literature. A later study identified risk factors as advanced AIDS, chronic sinusitis, neutropenia (a lower than normal count of white blood cells), or use of corticosteroids and prolonged use of broad spectrum antibiotics. There has also been at least one case of invasive aspergillus sinusitis in a long-term anabolic steroid user. Depending on the severity, treatment can range from antifungal medications to surgical intervention.
Severe Asthma with Fungal Sensitization (SAFS)
Patients with severe asthma are often on high doses of steroids, and both of these facts can lead them to be more sensitive to fungus — including Aspergillus species. They don’t meet the full diagnostic criteria for ABPA, and are instead diagnosed with SAFS. A conservative estimate of those with SAFS is around six million people, which represents the fact that severe asthma affects 5–20% of those with asthma,and of these, 35–50% have SAFS. Because severe asthma is a debilitating disorder that causes frequent medical contact and need for treatment, it is difficult to estimate the overall impact of SAFS. While it is theorized that this affliction can cause many intensive care unit hospitalizations and deaths, it is difficult to truly know the reach and impact of SAFS. Oral medications such as itraconazole can help reduce use of corticosteroids, but the required amount of time patients must use antifungal therapy to treat this illness is unknown.
Cutaneous Aspergillosis (Primary and Secondary)
Primary cutaneous aspergillosis (PCA), a relatively rare issue, often occurs at the site of burns, catheters, regions of traumatized skin — like what happens near adhesive bandages. It can also occur in trauma patients or at sites of surgical wounds by direct inoculation of Aspergillus spp. Meanwhile, secondary cutaneous aspergillosis (SCA) occurs by direct spread lungs or paranasal sinus, or by the blood. PCA and SCA is most often seen in burn victims, newborns, cancer patients, transplant recipients (of both bone marrow and organs). There is a general lack of literature about PCA / SCA in immunocompetent patients as it is believed to rarely impact them. In order to fully diagnose it requires a skin biopsy.
Because it is often a secondary infection, it’s important that pulmonary aspergillosis patients be monitored for any skin wounds, and that any skin sites where bandages and adhesives are closely watched.
Aspergillus Endophthalmitis
Aspergillus infections of the eye are most often observed after eye surgery, and can lead to significant vision loss and blindness. Because anti-fungal agents rarely are able to impact the eye in an effective dose, general prognosis is poor for patients who contract it. While there are many fungi that can impact the eye after surgery, Aspergillus is the most common. Treatment can include everything from local treatment to surgical intervention. It is most often seen in those who have received cataract surgery(which represents a low percentage of cataract patients overall), but it can also affect 30–40% of those with open-globe injury (where trauma is inflicted directly on the eye). It is also believed that introvitreal (injection into the eye) amphotericin B might be toxic to the retina.
Pulmonary Aspergillosis
As we have discovered together, pulmonary aspergillosis, particularly invasive pulmonary aspergillosis (IPA), gets a lot of attention in the community and in literature. Essentially, to map out the possibilities of pulmonary aspergillosis and its related diagnoses, M. Kousha, R. Tadi, A.O. Soubani included the following chart in their work, “Pulmonary aspergillosis: a clinical review” which was published in 2011 in the European Respiratory Review. It shows the common infection type split out by common comorbidities.
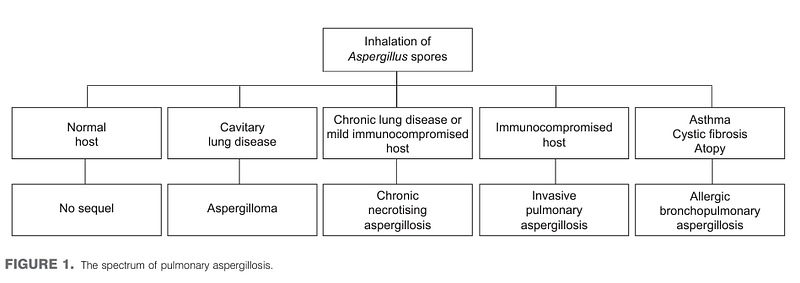
Clinically, these patients most often present with shortness of breath, a productive cough (in the more serious infections the cough can include blood), and in the case of invasive pulmonary aspergillosis, other indications such as high fever and chest pain.
Allergic Bronchopulmonary Aspergillosis (ABPA)
Primarily (but not exclusively) affecting patients with bronchial asthma or cystic fibrosis, ABPA is a type of fungal infection of the lung. The thick mucus in the airways of the patients make it difficult to clear out the fungal spores. Allergy to Aspergillus is tested for by skin prick sand up to 25% of asthmatics and 50% of cystic fibrosis patients test positive for this allergy. Estimations of state that 2- 13% of asthmatics and 1–15% of cystic fibrosis patients have ABPA. It is also often seen in those with atopy, a condition that is characterized by heightened immune responses and a genetic tendency to develop allergic diseases. ABPA is still not fully understood, but patients with sensitization to Aspergillus had more severe airflow obstruction and had more prescriptions for corticosteroids. Another misunderstood aspect is the link between ‘environmental load’ (the amount in the environment) and ABPA — and thus it’s highly important to test asthmatics and cystic fibrosis patients for this allergy. Treatment includes oral or aerosol steroids(especially during attacks), or itraconazole (an oral antifungal drug), which reduces the amount of steroids required in those needing higher doses.
The symptoms are very similar to asthma, and include wheezing, coughing, feeling unwell, and sometimes a cough that produces brown-colored mucus plugs. Symptoms will not respond to standard antibiotics and diagnosis can be made by x-rays, sputum samples, or blood tests. It’s also worth noting that some patients have Aspergillus allergies that are so serious they can go into anaphylactic shock. This allergic sensitivity can also induce asthma attacks, which kill about 10 people per day in the US.
Aspergilloma
Aspergilloma is considered to be non-invasive in that it is found in one part of the body, vs. invasive aspergillosis which is a more widespread infection. Aspergilloma is a fungal ball (mycetoma) composed of Aspergillus hyphae, cellular debris, and mucus. It is normally associated with patients that have underlying lung disease, chronic debilitating conditions such as malnutrition or liver disease, or immunosuppression. Treatments often include surgery, but post-surgical complications are frequent. Aspergilloma are found in approximately 25% of patients with chronic pulmonary aspergillosis. There are also cases of aspergillosis that is not in the lung (extra-pulmonary). While endocarditis caused by fungus is relatively rare (only 2% of cases), Aspergillus accounts for up to 25% of those cases. The most common indicator of pulmonary aspergilloma is hemoptysis — where the patient begins coughing up blood, which is a symptom recorded in 50–87% of cases.
Chronic Pulmonary Aspergillosis (CPA)
First recognition of chronic pulmonary aspergillosis as a fatal condition happened in Edinburgh 1842 by J. H. Bennett. Pulmonary aspergillosis as a term / condition was first described in 1959. Since then more clinical understand of the condition has evolved, especially as medical science advanced. The most common form of CPA is chronic cavitary pulmonary aspergillosis (CCPA), which describes when gas-filled pockets appear. If untreated, CCPA can turn into Chronic Necrotizing Pulmonary Aspergillosis. We are still learning about CNPA, a condition which is associated with high mortality due to the ongoing CCPA infection. CNPA causes not only lung damage causing cavitary lesions, but also evidence of aspergillus infiltration outside / near these spaces (paracavity infiltrates). Over time, new cavitary lesions will form, or the cavities created will expand.
Invasive Pulmonary Aspergillosis (IPA)
The most common people afflicted with IPA are stem cell transplant or organ (especially lung) transplant recipients, patients with hematologic malignancies such as lymphoma, myeloma, and leukemia, patients with prolonged neutropenia (low on a type of white blood cell), patients who are critically ill and in an intensive care unit, steroid use, patients on dialysis, liver disease patients, people with Chronic obstructive pulmonary disease (COPD) and other chronic lung diseases, and those with chronic granulomatous diseases, a disorder where white blood cells can’t effectively kill some fungi / bacteria. First described in 1953, IPA became more widespread due to use of chemotherapy and immunosuppressive agents. It has become increasingly more common over the past decades. One study found that in autopsies performed between 1978 and 1992, IPA increased from 17% to 60% of all fungal infections found. The mortality rate of IPA exceeds 50% in patients with neutropenia, and reaches 90% in haematopoietic stem-cell transplantation (HSCT) recipients.
There has been an increase in reports of immunocompetent patients who do not have the classic risk factors that contract IPA. In particular, patients with severe COPD and critically ill patients both have increased risk. It’s possible that patients with COPD have increased susceptibility to IPA for many reasons, including changes in the lungs, prolonged use of corticosteroids, frequent hospitalization, broad-spectrum antibiotic treatment, invasive procedures, and comorbid illnesses such as diabetes, alcoholism and malnutrition. IPA is also becoming a more prevalent disease in ICU’s, even in patients without the common risk factors. Studies of IPA in non-compromised hosts, especially those in intensive care, are increasing — a study in 2019 of patients autopsied found that IA is one of the most commonly missed diagnoses in critically ill patients, and of the 893 autopsies in the ICU, 25 (2.8%) were able to be diagnosed with IA, while only 10 of those had been diagnosed and put on antifungals pre-mortem.
Depending upon a range of risk factors, the mortality rate of IPA can be between 40 and 90%.
Risks
As stated in all of the above information, being immunocompromised, being treated with immunosuppressing drugs, using prescribed corticosteroids, COPD, asthma, cystic fibrosis, can all impact how Aspergillus exposure intersects with someone’s health. It’s also important to note that occupational exposure, especially in ‘high load’ situations (where there is a lot of aspergillus around) is a risk factor. Remember from our study of the history — in 1945 aspergillus was identified as a possible contaminant causing farmer’s lung.
Those aren’t the only risk factors, however — there are others that have been recently emerging in the literature.
Occupational Hazards of Aspergillus
There have been several papers addressing the occupational hazards of aspergillus, as our understanding of exposure to heavy loads of the fungus evolves. There are many papers exploring Aspergillus exposure as an overall occupational risk, and some of the papers cover the hazards of Aspergillus exposure in ceramics workers and the composting industry. One even acknowledges the link between occupational exposure to aspergillus and the rise in azole-resistant infections. ABPA has specifically been identified as a risk in waste management professions,and demolitions.
There are also many that identify fungal exposure in cannabis operations as a particular concern. A study in 2013 explored fungal spores in Indoor Marijuana Grow Operations, and it found that there was a shift in dominant spore type from Cladosporium sp. outdoors to Aspergillus sp./Penicillium sp.(Asp/Pen) in the grow rooms. Another 2015 paper explored cannabis allergies, and found urticaria (hives / welts) and other cutaneous symptoms from exposure to the cannabis itself (which is an interesting thing to note after learning about cutaneous aspergillosis) in a laboratory worker and a grower. Much of the documentation of the intersection of cannabis and aspergillus for occupational hazards references work we will discuss later in this article. One mentions that the environment that can be optimal for cannabis can also be optimal for fungal growth.
Aspergillosis and Influenza

Over the past several years, the incidence of aspergillosis patients with influenza has increased. In a recent multicenter study that encompassed seven influenza seasons, seven institutes demonstrated
influenza as an independent risk factor of IPA (adjusted odds ratio 5.19, 95% confidence interval (CI) 2.63–10.26,p < 0.001). The study, which covered the period between Jan 1, 2009, and June 30, 2016, found that 19% of the 432 patients were found to have invasive pulmonary aspergillosis. This study inspired a panel of 29 experts to define a new diagnostic category of aspergillosis — Influenza-assisted pulmonary aspergillosis (IAPA). The study stated, “Since IAPA may develop in a wide range of hosts, an entry criterion was proposed and not host factors.” It goes on to review the criteria for diagnosis with IAPA, stating that the patient was one that required ICU admission for respiratory distress, that they were positive for the flu, and that there was proven evidence of Aspergillus via one of several tests.
Aspergillosis and COVID-19
Building on the work to define influenza-assisted pulmonary aspergillosis, and faced with the medical implications of a pandemic, researchers and physicians recognized an intersection between COVID-19 and aspergillosis. In a literature review published in 2020, Chih-Cheng Lai and Weng-Liang Yu saw rates of IPA in COVID-19 patients that ranged from 19.6% to 33.3%. The patients did not have the typical risk factors associated with Aspergillosis. In 2020, a group of researchers and physicians came together to clinically define COVID-assisted pulmonary aspergillosis (CAPA). In studying a cohort of 108 critically ill patients with acute respiratory distress syndrome, patients with CAPA experienced higher 30-day mortality than those without aspergillosis (44% vs 19%). The paper proposes three different grades: possible, probable, and proven CAPA with recommended tests for identification and treatment. The conclusion of the study acknowledges that the general outlook and prognosis for patients with CAPA is poor, and that “Aspergillus can cause co- infection with SARS-CoV-2 despite these patients who did not have a traditional risk factor of Aspergillus infection.”
Aspergillosis and Cannabis
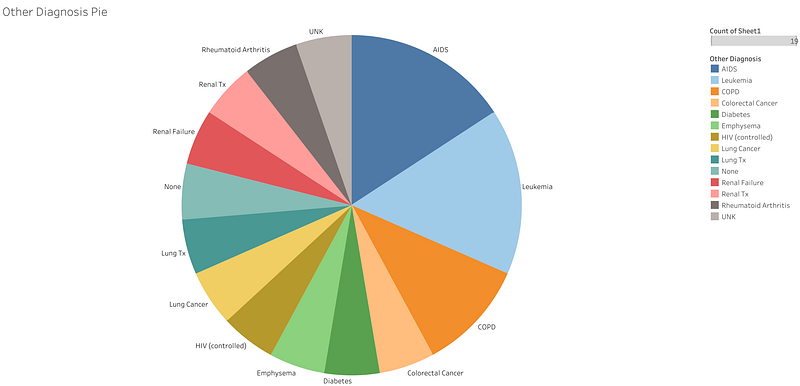
Now that we have an overall understanding of what illnesses Aspergillus can cause, we can finally explore what the medical literature says Aspergillus and cannabis. The summaries of these case studies are sorted by date in reverse chronological order. First and foremost it’s important to state the rarity that patients admit cannabis use to their physicians, which would be a prerequisite to being included in the medical literature.
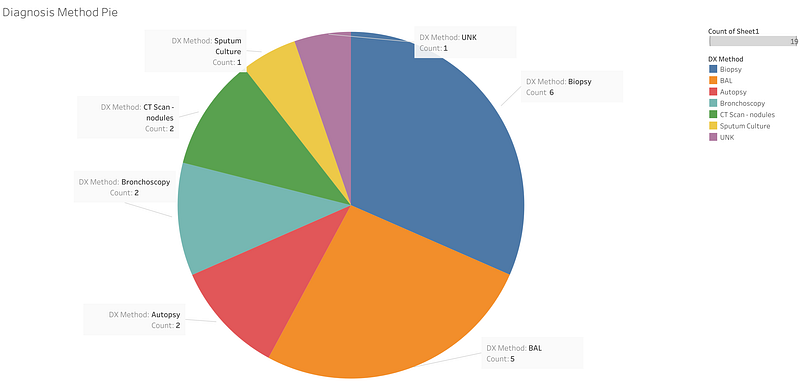
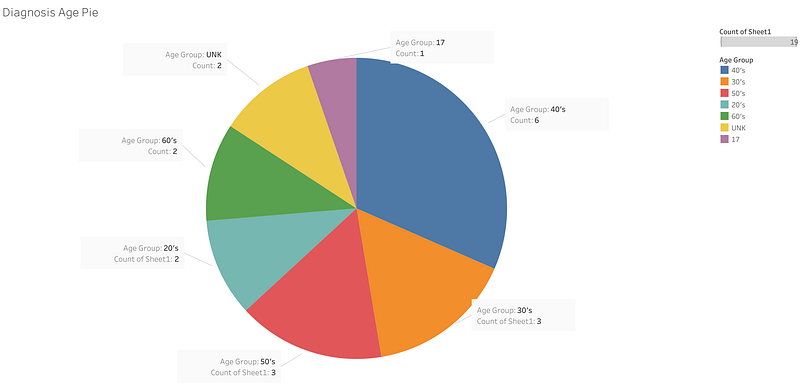
Overall there are several studies that I explore below, but it wouldn’t be me if I didn’t put some data together about them. You’ll see some summary information scattered through the text.
February 2022 Fatal Early-Onset Aspergillosis in a Recipient Receiving Lungs From a Marijuana-Smoking Donor: A Word of Caution by Eleonora Faccioli, Federica Pezzuto, Andrea Dell’Amore, Francesca Lunardi, Chiara Giraudo, Marco Mammana, Marco Schiavon, Antonello Cirnelli, Monica Loy, Fiorella Calabrese, Federico Rea
This letter, written to Transplant International, opens by commenting on the lack of study of the impact of donor’s cannabis smoking habits on lungs donated for transplant. The authors then recount a case of interest. A 50 year old transplant patient had received the donated lungs from a 21 year old donor. The donor had died of a traumatic brain hemorrhage, and the only remarkable aspect of his medical history was his cannabis use. His OTO score, a score which assigns points to donor factors such as age, smoking, etc. was 0 which is the ‘best’ possible, and microbiological tests are negative.
The lung transplant itself was relatively normal (as far as lung transplants go), and the patient was receiving the lungs due to his idiopathic pulmonary fibrosis, a condition in which the tissue surrounded the alveoli,the air sacs that allow for gas exchange between the lungs and the blood, becomes thick and stiff for unknown reasons.
Post-transplantation the patient was given aerosolized amphotericin B (an antifungal), ganciclovir (an antiviral used to treat cytomegalovirus, a a common lifelong viral infection which most people don’t realize they have but can have impacts for transplant patients and HIV patients) and two corticosteroids (mycophenolate mofetil, and cyclosporine). Bacteria was found in the blood culture and bronchial aspirates. Despite this, he was being considered for discharge as he had improved. The doctors decided one more bronchoscopy was necessary to perform surveillance, but the sample was insufficient and they determined that there was alveolar damage and organizing pneumonia, a condition caused by damage to the alveolar wall. There was also another issue, ischemia reperfusion injury, which is often due to tissue being damaged by the return of blood supply. There was no evidence of acute rejection, infection, nor were there marijuana-related lesions detected.
The following day, the patient was coughing up a lot of blood (hemoptysis), and went into cardiac arrest, which required reintubation and a return to the intensive care unit. Several more instances of hemoptysis occurred, and the patient died 10 days later due to hypovolemic shock (when your heart can’t get enough blood to your vital organs).
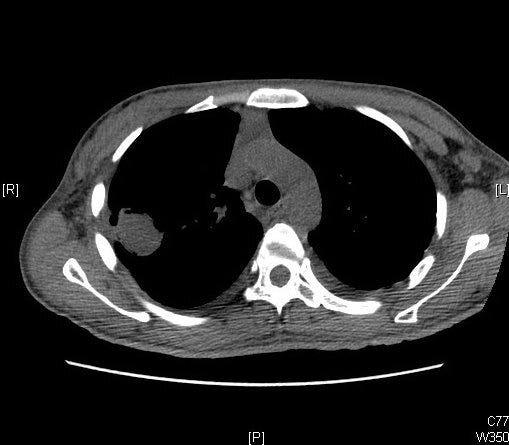
A CT scan had been performed before the patient died which showed bilateral nodules, possibly due to the hemoptysis, and a wedge-shaped nodule. Upon autopsy invasive pulmonary aspergillosis was revealed, in addition to smoking-related lesions.
It is believed that “this is the first report of fatal early onset IPA in a patient who received lungs from a donor with ongoing marijuana use.” The authors also suggest “In case of young donors with cannabis smoking history, the pre-emptive research of fungi (especially Aspergillus) on biological samples should always be encouraged. At the same time, more sensitive tools, like polymerase chain reactions, could help in the early detection of Aspergillus in recipients with bleeding unrelated to the surgical procedure undergone.”
August 2020: Invasive pulmonary aspergillosis in an immunocompetent, heavy smoker of marijuana with emphysema and chronic obstructive pulmonary disease by Vincenzo Zagà, Mohamed A. M. M. Abdelrazek, Sarah Shalhoub, Marco Mura
A 51 year old man with chronic obstructive pulmonary disease (COPD) and emphysema presented to a clinic in 2018. His progress and health had been monitored since 2013. When he presented in 2018 he complained of shortness of breath, fatigue, and weight loss. He had been smoking approximately 30 joints per day of pure cannabis (no tobacco). He also did not use any vaping devices. He was using a bronchodilator that included azithromycin, but no corticosteroids. He had the option of home oxygen therapy but was non-compliant with it.
He presented later to the Emergency department after 10 days of treatment with the antibiotic cefixime. His cough had worsened and was producing more yellow sputum than before. He wasn’t running a fever, but necessitated oxygen at 5L / minute, whereas before he required 3L / minute. He wasn’t running a fever but was fatigued.
His chest x-ray revealed a new area of opacity, possibly indicating gas-filled nodules (‘cavitation’) in the right upper lobe. Since he hadn’t responded to the cefixime, he was admitted and started on piperacillin/tazobactam, another antibiotic combination, and given a CT scan which revealed thick-walled, gas-filled spaces, which was possibly indicative of necrotizing consolidating pneumonia. For the next five days, the patient did not improve. Because of the emphysema a biopsy was deemed unsafe, so a bronchoscopy and bronchoalveolar lavage (BAL) was performed, which is a test where a lighted tube called a bronchoscope is put through the nose or mouth and run into the throat and airways — then a sterile saline solution is washed into the airways and suctioned back up for evaluation.
The BAL culture was positive for Aspergillus fumigatus. His immune status was confirmed to be normal, and further testing confirmed he was negative for HIV and Legionnaires disease. His immune status was confirmed to be normal, including white blood cell count.
The antibiotics were discontinued and voriconazole (anti-fungal) treatment was started with careful monitoring of his liver functions. In the 16 days he had been in the hospital, he had lost 15 pounds (7 kg). Voriconazole treatment continued for three months.
38 days after discharge, the patient developed a pneumothorax (abnormal air in the pleural space between the lung and the chest wall, which is also known as a collapsed lung) that was treated successfully with a chest tube.
Eventually on treatment with voriconazole, the patient regained function and weight, but confirmatory tests were performed to ensure that the patient did not have any sort of malignancy. Biopsies of the lymph node were taken, and another BAL test was completed which confirmed the lack of cancer, and the BAL, which was administered 74 days after the first, was negative for A. fumigatus. During this time the patient stopped using marijuana, and eventually his health returned to baseline.
The case was determined to be invasive pulmonary aspergillosis because of its rapid onset and acute nature (vs. chronic necrotizing aspergillosis).
In the discussion section of the case, the authors suggest use of edibles vs. smoked cannabis in order to mitigate risk, and that the use of gamma irradiation (as they do in Canada) may not be effective in protecting heavy users.
June 2020: Cannabis Use and Fungal Infections in a Commercially Insured Population by Kaitlin Benedict, George R. Thompson, and Brendan R. Jackson
The paper authors, who are from the Centers for Disease Control and Prevention and University of California Davis Medical Center, used the 2016 IBM MarketScan Research Databases to examine patient interactions for over 27 million 27 million employees, dependents, and retirees throughout the United States. Using International Classification of Disease codes (ICD10), they looked for information at the intersection of a history of cannabis use in addition to other diagnostic information.
According to the paper’s abstract, they found that persons who used cannabis were 3.5 (95% CI 2.6–4.8) times more likely than persons who did not use cannabis to have a fungal infection in 2016.
“Persons who use cannabis were more likely than persons who did not use cannabis to have mold infections (0.03% vs. 0.01%; OR 3.4, 95% CI 2.1–5.3, aOR 4.6, 95% CI 2.9–7.4) and other fungal infections (0.04% vs. 0.02%; OR 2.2, 95% CI 1.4–3.3, aOR 2.9, 95% CI 1.9–4.5)… Among patients with fungal infections, persons who used cannabis were significantly younger than persons who did not use cannabis (median age 41.5 years vs. 56.0 years; p<0.001), more likely to be immunocompromised (43% vs. 21%; p<0.001), more likely to be hospitalized on the fungal infection diagnosis date (40% vs. 13%; p<0.001), and more likely to have tobacco use codes (40% vs. 9%; p<0.001)”
Aspergillosis has a specific ICD-10 Code section, B44, and these codes were used in addition to cannabis use codes in the database. It is noted that cannabis use is often ‘greatly’ underreported to physicians by patients. The table of data is here, and it shows that the greatest incidence of fungal infection in cannabis users that were part of the research is for Aspergillus.
August 2017 Disseminated aspergillosis in an HIV-positive cannabis user taking steroid treatment by Salam, Alex P; Pozniak, Anton L
A 47 year old woman presented to the hospital with confusion and seizures. She had well-controlled HIV (her blood had the same amount of T-cells as someone without HIV, CD4>1000, and an undetectable viral load). She was administered a brain MRI, which was ‘unremarkable’ Her cerebrospinal fluid had a high amount of lymphocytes (which often indicates infection), high protein levels (which can indicate a tumor, blockage, or nerve inflammation), and low glucose levels (another indication of illness). CT chest images showed cavitating lesions in the left lobe of the lung, but there were also ‘tree-in-bud’ opacities which are associated with tuberculosis.
She was started on tuberculosis treatment which included dexamethasone, a corticosteroid, and followed up with physicians appropriately. The diagnosis of tuberculosis was confirmed when Mycobacterium tuberculosis grew from samples from her bronchoalveolar lavage (BAL, a test where saline is washed into the airways and then retrieved for sampling).
But she presented again at the emergency department after 2 days of running a fever, coughing blood, and drowsiness. Her Glasgow Coma Score, which is used to score patients based on their ability to move their eyes, respond verbally, and motor responses, gave her 10 overall. 4 for her eyes (meaning she could open them and close them on her own), 1 for verbal (she couldn’t speak or make sounds), and 5 for motor (meaning she could move away from pressure, but is not the full score of 6, which indicates an ability to follow where and when to move).
A chest CT showed that the lesions in the left lobe of her lung had shrunk, but new ones had appeared in the right upper lung and the left lower lung. Brain MRI showed multiple lesions. When a biopsy was performed on the right upper lobe of the lung, it revealed fungal hyphae, and she started on amphotericin B (450 mg daily). A. fumigatus grew from both the biopsy sample and the BAL sample.
A day after admission, her Glasgow Coma Score dropped to 8 — her pupils became fixed and dilated. She died a day later. Subsequent conversations with her family revealed that she was a heavy cannabis user. The case study authors believe that though her HIV was well-controlled, the combination of dexamethasone possibly creating an immunosuppressive state and repeated Aspergillus exposure via her cannabis use contributed to her death.
March 2017 Aspergillosis Presenting as Multiple Pulmonary Nodules in an Immunocompetent Cannabis User by Tara M. Babu, Matthew K. Griswold, Marguerite A. Urban, and Kavita M. Babu
A 46 year old man presented to the Emergency Department complaining of left-side weakness and loss of coordination (ataxia). He had a history of high blood pressure, but did have a chronic cough. He denied symptoms such as fever, chills, weight loss, loss of appetite, or any additional respiratory issues. The only issues that arose during his physical exam confirmed left-sided weakness (hemiparesis), and rapid eye movement (nystagmus). To rule out cerebrovascular disease or tears in the arteries, a CT angiogram, which is a test meant to examine the health of the arteries supplying the heart — but in this case pulmonary nodules were discovered. After the resolution of his symptoms he was discharged, and the experience was attributed to transient ischemic attack (colloquially known as a mini-stroke).
The lung nodules, however, were examined over the next few months. A CT-guided biopsy showed atypical cells, inflammation, and white blood cells that were loaded with a protein that stores iron (hemosiderin), which can be indicative of damage to the alveoli, the tiny air sacs responsible for exchanging carbon dioxide and oxygen in the bloodstream. His family was braced for a cancer diagnosis when he was referred to a surgical clinic for video-assisted thoracoscopic surgery and a wedge biopsy.
Instead, the biopsy revealed a large fungal ball with characteristics consistent with Aspergillus species. It was determined that the patient did not have prior lung disease — no tuberculosis or COPD. He hadn’t had any occupational risks or exposures, and recent HIV tests were negative. He had no underlying immune deficiency. He did engage in daily, heavy alcohol use, was a smoker, and smoked ‘one pipe a day’ of marijuana.
The patient was given a treatment plan that included a loading dose (400 mg two times a day) and then daily doses (200 mg twice daily for a month) of voriconazole. The patient was counseled on the importance of quitting alcohol during the anti-fungal treatments. He was ‘lost to follow-up,’ which means he skipped out on his follow-up visits, but physicians were able to reach him by phone and confirm that his issues had resolved.
The study mentioned that “While contaminated tobacco contained 200–300 colony-forming units per gram (CFU/g) of mold, the contaminated marijuana had 10,000–10,000,000 CFU/g. Other opportunistic molds were also identified in the marijuana samples, including Penicillium, Fusarium, Acremonium, Rhizopus, and Scedosporium species.” It emphasized “Patients who smoke cannabis to relieve chemotherapy-induced nausea may be at particularly high risk.” It also explicitly reinforced that cannabis use is a risk for Aspergillosis.
November 2015: Chronic necrotizing pulmonary aspergillosis in a patient with diabetes and marijuana use by Tamara Leah Remington , Jeffrey Fuller, Isabelle Chiu
Chest pain and shortness of breath brought a 29 year old with type 1 (juvenile) diabetes to the emergency room. While initially the patient did not think they had any other symptoms, he did recall night sweats, fever, weight loss, and a general feeling of being unwell for around a year. In addition to insulin, the patient was taking a proton pump inhibitor, which inhibits proton pumps from producing too much acid in the stomach (pantoprazole). The patient vaporized cannabis, acquired from the same dealer from the illicit market, daily for diabetic neuropathy for the last 18 months in addition to occasional oxycodone.
Around 18 months prior to admission was when initial symptoms of neuropathy presented, and he had this experience for around 6 months before being diagnosed with diabetes (around a year prior to admission). At that time he was also found to have diabetic retinopathy. Two months later (and 10 months before his presentation at the emergency room), he had been diagnosed with community-acquired pneumonia, and had evidence of abnormal growths (infiltrate) in the lower-left lobe of his lungs. No follow up x-rays were taken. Computerized tomography of his abdomen that was performed for unrelated issues did reveal evidence of ongoing issues in the lower left lung (consolidation). Physical examination was relatively normal except for evidence of decreased air entry to the base of his left lung.
A radiograph and computerized tomography of the lungs showed a pneumothorax and air space disease in the lower left lung. A chest tube did not relieve the symptoms. Video-assisted thoracoscopic surgery showed diffuse pleural adhesions. As the surgery was both diagnostic and therapeutic, decortication (removal of fibrous tissues around the lung) and a wedge resection (removal) of some of the lower left lung tissue was performed.
The tissue samples from the wedge resection grew a Penicillium species, a non-sporulating fungus…and A. fumigatus. Blood tests were largely normal, and revealed that the patient’s immunoglobulins (antibodies) were also normal except for a mildly low level of immunoglobulin G4, which can indicate infection in the respiratory system, stroke in the circulatory system, or possible damage to the kidneys in the urinary system.
The pneumothorax was resolved after surgery and the patient was given a six month course of voriconazole, an oral medication for serious fungal or yeast infections. His symptoms resolved, and the resolution was confirmed by radiography tests. Cultures from his cannabis grew Penicillium species, Aspergillus versicolor and Aspergillus ochraceus. His vaporizer, however, did not grow any fungal species.
It is believed that the fungal infection began one year earlier, when the patient had been diagnosed with diabetes — the presence of retinopathy and neuropathy might indicate the patient had a prolonged period of hyperglycemia. Diabetes is a mild immunosuppressive disease, which makes it a risk factor for chronic necrotizing pulmonary aspergillosis.
This case study caused two responses from other Canadian doctors.
January 2011 TOO MANY MOULDY JOINTS — MARIJUANA AND CHRONIC PULMONARY ASPERGILLOSIS By Yousef Gargani, Paul Bishop, and David W. Denning
This covers the case history of two patients who contracted chronic pulmonary aspergillosis through cannabis use. Both of these patients sought treatment in the United Kingdom.
The first patient, a 47 year old male presented with right-sided pneumothorax (collapsed lung). For the prior four years he had been experiencing increased breathlessness. He was a 39 pack year smoker (meaning he smoked a pack a day for 39 years or the equivalent, like 1.5 packs a day for 26 years, etc.). He began to smoke marijuana medicinally, which is when his symptoms began to worsen. At the time he sought help he was coughing up thick sputum and had lost weight. He was taking a daily 5 mg dose of a corticosteroid / hormone steroid and 1 mg of Sulfasalazine, an antirheumatic drug, which he took twice daily. The patient had rheumatoid arthritis, which is why he was smoking 5 joints a day — to relieve the pain from rheumatoid arthritis.
Despite draining, his condition did not improve, and a bullectomy and pleurectomy was performed. A bullectomy is surgical removal of a bulla, a dilated air space within the lung — the most common cause of which is COPD, or chronic obstructive pulmonary disease. A pleurectomy is the partial removal of the pleura. A bulla that was removed contained an aspergilloma, a fungal ball made of Aspergillus hyphae, cellular debris, and mucus — and the picture included shows around a 7 cm mass.
He continued to have issues and CT scans showed emphysema and additional lung complications. Because of the discovery of the aspergilloma, he was placed on an anti-fungal medication, posaconazole twice a day for four months. After this, his symptoms improved. He stopped smoking marijuana and was observed for 4 years following his illness, and there was no evidence found of a recurrence.
The second patient was a 35 year old male who had shortness of breath. He also had a viral infection, and had a rare condition called a ‘Tetralogy of Fallot,’ which is a combination of four defects of the heart that causes oxygen-poor blood. Infants and children with the condition have blue-tinged skin due to the condition, and it requires corrective surgery and regular checkups with physicians for the rest of the patient’s life. This patient’s surgical repair happened at the age of 10, and it caused him a great amount of postoperative pain. Eventually he sought something to relieve the pain, and found that marijuana did the trick.
He grew his own cannabis, and despite the UK tendency to mix marijuana and tobacco, he didn’t — instead smoking straight cannabis.
At his initial visit, when he was 35, he was diagnosed with emphysema. He went on with his life for around 8 years, when he turned up again as a 43 year old patient complaining of breathing issues, and then multiple more times due to respiratory failure. When he turned 44, he stopped the 34 year old habit of 20 joints a day. Despite quitting, he still continued to get sicker, until he was feeling exerted with very little exercise at all (’10 yards on the flat.’)
Even with 3L continuous oxygen, his blood oxygen levels stayed around 91% (healthy levels are between 95 and 100 percent). A CT scan showed that there was severe panlobular (panacinar) emphysema that involved the right upper and middle lobes. There were also cavitary lesions that appeared to be aspergilloma, and a sputum culture was positive for A. fumigatus. His blood revealed antibodies for Aspergillus, and his respiratory function grew so bad he required a lung transplant — but the discovery of an aspergilloma was a huge impediment to that operation. Doctors started him on 200mg of voriconazole twice a day, but four months later, he died at the age of 45.
There are several interesting comments made in the discussion section. “The way marijuana is smoked is different… joints are… usually smoked without a filter and are smoked down to a smaller butt. Users hold their breath for longer and use the Valsalva maneuver… in doing so however, they expose their lungs to a greater tar and carbon monoxide burden, as well as subjecting their lungs to greater pressure changes. This barotrauma from marijuana smoking has long been associated with the formation of bullae and subsequent pneumothoraces. The association is so strong that some now recommend that patients presenting with spontaneous pneumothorax should be directly questioned about marijuana smoking.” They also comment, “It has been reported that 44% of US oncologists have recommended the illegal use of marijuana to their chemotherapy patients for iatrogenic nausea. What must be borne in mind is that these patients are potentially severely immunosuppressed and therefore at risk of life-threatening IA.”
February 2010, Chronic necrotising pulmonary aspergillosis in a marijuana addict: a new cause of amyloidosis by Bal, Amanjit; Agarwal, Ashutosh Nath; Das, Ashim; Suri, Vikas; Varma, S.C.
A 32 year old male had an intermittent fever for 1 month, in addition to reduced urination and swollen legs and ankles when he presented to a private hospital. He was catheterized and received peritoneal dialysis, which increased urination. 5 years prior, he had been coughing up blood, which was treated for 7–9 months with anti-tubercular treatments. Since that episode, he continued to have a slightly productive cough which increased over the last two months. He was a chronic tobacco smoker for 15 years, occasional drinker — and, as the paper calls him, ‘a marijuana addict’ (they mention he had withdrawal symptoms during his stay at the private hospital).
He didn’t have a fever, had a heart rate of 90, and a chest x-ray revealed that his lungs had healed scars (fibrotic lesions) and a few soft infiltrates on both sides. His ultrasound showed that he had renal parenchymal disease (which is any disease which affects the filtration part of the kidneys, ‘parenchyma’ means the functional tissue of an organ). Fine needle aspiration was positive for amyloids, and the patient was diagnosed with chronic renal failure.
While his initial urine output had been 1 L / day with hemodialysis, his output became 700 mL / day with alternating day dialysis. While his physicians wanted to perform a biopsy, his increasing cognitive impairment delayed that.
Unfortunately, the patient died of cardio-respiratory arrest before fresh dialysis could be planned.
During autopsy his lungs were examined, and found to be heavy (1500g), and both upper lobes were fibrotic. There were nodules, hemorrhaging, and bullae. A cavitary lesion was found and upon examination fungal hyphae’s presence. But — there was no evidence of healed or active tuberculosis. The spleen, thyroid, adrenals, and liver all showed evidence of amyloid. After all of the tests and examinations were complete, the patient’s autopsy revealed chronic necrotising pulmonary aspergillosis with secondary systemic amyloidosis, which his doctors believed was caused by his chronic marijuana use.
May 2008 Invasive pulmonary aspergillosis associated with marijuana use in a man with colorectal cancer by David W Cescon , Andrea V Page, Susan Richardson, Malcolm J Moore, Scott Boerner, Wayne L Gold
Two years before this paper was written in 2006, a 65 year old man with a history of colorectal cancer appeared for an oncology follow-up complaining of cough, fever, and difficulty breathing especially when exerted. His diagnosis of colorectal cancer occurred two years before his 2006 visit, and was treated with resection (removal) and chemotherapy. Nine months later he was treated for metastatic disease (the cancer spread) of the lung and pelvis, and had completed eight months of chemotherapy which was effective in reducing the tumor. During the followup, they decided to postpone the ninth scheduled chemotherapy treatment, and was instead prescribed treatment for a bacterial infection. His symptoms worsened, and he started to cough up small amounts of blood at which point he presented to the emergency department for evaluation and treatment.
He had no notable medical history, had never been exposed to tuberculosis, and didn’t smoke cigarettes. He had started smoking marijuana to relieve the nausea from chemotherapy six weeks before presentation to the emergency department. Cultures of blood and sputum were negative for bacteria, mycobacteria, and fungi. A CT scan revealed a cavitary lesion in the lung, and when a CT-guided fine needle aspiration biopsy (they used imaging to guide a needle to pull some fluid) was performed, fungal hyphae compatible with Aspergillus was found, along with plant matter (presumably some cannabis). There were no malignant cells.
The patient was given a standard three month course of voriconazole, and in six months was clear of all symptoms (and confirmed with radiography).
February 2008 A 56-year-old woman with COPD and multiple pulmonary nodules by Ammar Sakkour, Tisha Wang, Donald Tashkin
A 56 year old woman with a history of COPD was referred to a pulmonology clinic. She was a ‘30-pack-year’ smoker (meaning she either smoked a pack a day for 30 years or the equivalent — 1.5 packs a day for 20 years, etc.). She had quit the tobacco cigarette habit 8 years prior, but had continued daily smoking of marijuana cigarettes for the last 10 years. She was referred due to nodules on the upper left lobe of the lung, but wasn’t experiencing cough, fever, night sweats or other symptoms. She did experience exertion-based labored breathing (dyspnea), but it was unchanged from her prior baseline values.
Her COPD had been diagnosed three years earlier based on pulmonology function tests and a CT scan of her chest. Her only medication use was of over the counter nasal sprays and hormone replacement therapy. There were no other risk factors present — no HIV, no occupational hazards, and no recent travel. She had been sent to have a CT-guided aspiration (needle biopsy) of the nodes in the upper left lobe of her lung. The first aspiration showed necrotic tissue but no cancer, and a second was performed which was also inconclusive. A bronchoscopy with BAL (a test where sterile saline is run into a part of the lung and collected for testing via suction) also came back inconclusive, though there was one colony of Candida albicans, which was considered ‘clinically insignificant.’
She was then admitted to the hospital, and had thoracoscopic surgery, where a biopsy was taken. This test was the one that allowed the diagnosis of invasive pulmonary aspergillosis. The researchers stated, “To our knowledge, this is the first documented case of invasive pulmonary aspergillosis associated with marijuana smoking in a patient without clinical evidence of an immune deficiency.” They acknowledged another case in which an otherwise healthy 23-year-old had a fungal element in the pathology, but in this case the fungus was fully identifiable as Aspergillus.
Initial treatment with Amphotericin B caused too much nausea and renal damage for the patient, who instead received a three month treatment with itraconazole. Follow-up radiography of her chest showed reduction of the nodules in her lungs, and she eventually recovered.
February 2001: Early invasive pulmonary aspergillosis in a leukemia patient linked to aspergillus contaminated marijuana smoking by M Szyper-Kravitz, R Lang, Y Manor, M Lahav
This paper details the medical case of a 46 year old patient who presented with fever, chills, and a dry cough. He was started on broad-spectrum antibiotics. His x-rays and physical examination came back normal, but his hematological evaluation revealed acute myeloid leukemia, and induction therapy (aimed at reducing the number of plasma cells) was started in addition to antibiotics. His condition began to worsen, with spiking fever, chills so bad they shook his body, rapid breathing, and low levels of oxygen in the blood (hypoxemia). Blood and sputum samples came back negative for bacteria and fungi. A chest CT indicated abnormal growths (focal nodular infiltrates) in the lung.
An investigation of the patient’s circumstances revealed that the patient smoked daily from a hookah mixing tobacco and cannabis. While waiting for the results of legionella and fungi tests performed on cultures from the hookah water and tobacco, physicians started the patient on antifungal therapy with amphotericin B. The fever and hypoxemia resolved after 72 hours on the medication. The cultures taken from the tobacco / cannabis mixture came back positive for heavy growth of ‘Aspergillus species’ (the exact species was unspecified).
The authors state: “We suggest that habitual smoking of Aspergillus-infested tobacco and marijuana caused airway colonization with Aspergillus. Leukemia rendered the patient immunocompromised. . . Physicians should be aware of this potentially lethal complication of “hookah” and marijuana smoking in immunocompromised hosts.”
June 1996 Successfully treated invasive pulmonary aspergillosis associated with smoking marijuana in a renal transplant recipient by W H Marks, L Florence, J Lieberman, P Chapman, D Howard, P Roberts, D Perkinson
This case is about the successful treatment of a transgender woman (46 years old). She developed end-stage renal disease at the age of 34, related to glomerulonephritis (a grouping of issues related to swelling of the filters in the kidneys, called glomeruli. She was on dialysis for 14 years waiting for a renal transplant. She was Cytomegalovirus positive (CMV). Cytomegalovirus is a common virus that infects a person for the entirety of their life (but often people are unaware they even have it), but was able to have a renal transplant from a CMV positive donor cadaver, and was on several post-operative immunosuppressive drugs.
She was discharged six days post-operatively. Four weeks after transplantation the patient was readmitted with 24 hours of non productive cough, a fever of 100.2, lethargy, and weight loss. The initial chest x-ray didn’t show anything, bacterial and viral tests came back negative, but her sputum had branching hyphae in it.
Her treatment initially was 400 mg itraconazole 4 times daily and a reduction in the prednisone that was given post-operatively, which caused some improvement. However, an x-ray indicated that there was an issue in the right upper lobe, and a CT scan revealed necrotic nodules there. A bronchoscopy showed mucus-containing plaques that extended from the vocal cords into the right mainstem and upper lobe. Hyphae consistent with aspergillosis was present in washings taken from the bronchoscopy, and biopsy confirmed invasion into the bronchial wall.
Doctors continued to down-adjust immunosuppressant medication, but in those three days the patient worsened, so the patient was put on IV amphotericin B colloidal dispersion (called ABCD). This therapy continued for six weeks, and the last two weeks were administered as an outpatient. The efficacy of this treatment was confirmed by normal chest x-rays. Though her renal function deteriorated slightly through the ordeal, it returned to normal after she finished ABCD therapy.
When Aspergillus risks were investigated, she denied routes of exposure other than marijuana. She revealed habitual use which she had resumed on postoperative day 6, and when the remaining marijuana was tested, it was positive for mixed Aspergillus species.
One year after her renal transplant and her infection, she continues to do well, is still on immunosuppressive regimen, is a stand-up comedienne, and lives an active life.
March 1991 Pulmonary Aspergillosis in the Acquired Immunodeficiency Syndrome by David W. Denning, M.B., B.S., Stephen E. Follansbee, M.D., Michael Scolaro, M.D., Stephen Norris, M.D., Howard Edelstein, M.D., and David A. Stevens, M.D.
This article is focused on the impacts of pulmonary aspergillosis in AIDS patients, and reviews 13 cases overall, some in summary, and a couple of them in detail. 13 of the patients had HIV and 12 of them had AIDS. Aspergillosis was detected a median of 25 months after diagnosis with HIV, and 10 of the patients died a median of 3 months after diagnosis (the range was 0 to 12 months). 10 of the patients had invasive aspergillosis, and 3 of them had obstructive aspergillosis (and those three coughed up fungal casts).
The patients were all men, and some of them had multiple risk factors for aspergillosis. Four of them used marijuana, three of them regularly, but seven of the patients didn’t have marijuana use noted.
Only two of the patients were explored in-depth and only one of the cannabis patients, known as patient 11. Patient 11 was 37 in August 1987 when he developed P. carinii pneumonia. He also had esophageal candidiasis and upper gastrointestinal bleeding a month later. Chronic perineal herpes led to the formation of a rectourethral fistula. This caused several episodes of urosepsis which was treated with an antibiotic, ciprofloxacin. The patient discontinued their use of alcohol, but continued to use marijuana.
In April of 1989, the patient was admitted due to shortness of breath and increased incidence of a dry cough. He reported a fever which was 105 degrees F (41 C). His white blood cell count was low (leukopenia) a chest film showed fluffy lower-lobe infiltrates on both sides. Despite being treated with two antibiotics (trimethoprim–sulfamethoxazole) his condition worsened, and a bronchoscopy was performed on day six of his admission. A foreign body was removed from the lower left lobe, and it was found to contain fungal hyphae of A. fumigatus.
He was put on 200mg of itraconazole, an antifungal, twice daily. After four weeks the sputum culture no longer showed A. fumigatus, and six weeks after the chest x-ray returned to normal. Regardless of the improvement, the patient’s urosepsis continued to worsen. Nine weeks after the discontinuation of the anti-fungal, the patient died of progressive dementia complicated by recurrent pneumonia and sepsis. No post-mortem was performed.
August 1988 Fatal aspergillosis associated with smoking contaminated marijuana, in a marrow transplant recipient. by Randa Harnadeh, M.D.; Abbas Ardehali, M.D.; Richard M. Locksley, M.D.; and Mary K. York, Ph.D
A 34 year old bone marrow transplant patient 75 days after his allogeneic bone marrow transplant for chronic myelogenous leukemia (CML), a relatively rare type of cancer (around 15% of leukemias) that impacts immature versions of myeloid cells — the cells that make red blood cells, platelets, and most types of white blood cells (except lymphocytes). In addition to total body irradiation, he received chemotherapy, and was on both cyclosporin (an immunosuppressant) and corticosteroids. He did experience complications, specifically graft vs. host disease which had been treated with high doses of steroids. 39 days after his bone marrow transplant, he was healthy enough to be discharged.
The patient remained healthy until two and a half months after his transplant, when he suffered two tonic-clonic (grand mal) seizures. A lumbar puncture (spinal tap) and brain CT revealed nothing. MRI of the brain showed two parietal nodules, and a chest x-ray revealed several nodules, some of which were cavitary (indicative of a gas-filled space). The patient’s bronchoalveolar lavage (BAL) didn’t indicate anything initially, but the patient was started on intravenous amphotericin-B. At this point an open-lung biopsy was performed, where fungal hyphae were found. Eventually the cultures from the BAL also grew A. fumigatus. The patient was also found to have cytomegalovirus, a lifelong viral infection. After further questioning of the patient, it was found they used cannabis daily prior to his admission. When the patient’s marijuana was tested it was also positive for A. fumigatus.
Unfortunately, even though they attempted a very aggressive treatment by adding an experimental antifungal drug, the patient developed pneumonia, then cholestatic jaundice, required intubation, and eventually died.
In the discussion section the authors relate the difficulty of diagnosis — that sputum cultures can be positive in up to 30% of patients and is only useful in certain subgroups, and that the only definitive way at the time was via lung biopsy. They warned physicians who were working with immunocompromised patients to be aware of the lethal implications of the experiences of this patient.
June 1986 Allergic bronchopulmonary aspergillosis associated with smoking moldy marihuana
The abstract of the paper that is available simply states “A 27-year-old man who habitually smoked marihuana developed clinical, laboratory, and radiologic findings consistent with allergic bronchopulmonary aspergillosis. Culture of the marihuana obtained from the patient’s source yielded heavy mixed growths of Aspergillus. Treatment with corticosteroids was effective.”
I can not find the full text of the paper to review to find if the patient was immunocompromised, and it’s perplexing that ‘treatment with corticosteroids was effective,’ when they so often put a patient at risk for aspergillosis, but as I said in the opening — I’m not a doctor. It’s worthwhile to note that ABPA, unlike IPA, is often treated with steroids.
April 1986: Possible risk of invasive pulmonary aspergillosis with marijuana use during chemotherapy for small cell lung cancer by Sharon Sutton, Bert L. Lum, and Frank M. Torti
A 60 year old with a history of limited stage small cell lung cancer presented at the hospital with skin lesions, 80 pound weight loss, and ‘progressive debilitation.’ 15 months prior to the hospitalization the patient had been diagnosed with a node on his lung, but before that he had enjoyed good health. The small cell lung cancer, limited to the upper lobe of the right lung and a regional lymph node, was treated by removal of the mass, chemotherapy, and prophylactic cranial radiation. The patient’s side effects of nausea, vomiting, and weight loss were not controlled by standard pharmaceutical protocols, so after six cycles of chemotherapy the patient began smoking three to four ‘marijuana cigarettes’ a day to find relief through the rest of his treatments.
Two months before presenting to the hospital, his treatment was considered complete, which was after 12 cycles of chemotherapy. Ten days before he was admitted, fluid filled sacs (cutaneous vesicles) started to appear, thought to be herpes zoster. Two days before he arrived at the hospital cutaneous lesions appeared on his torso and extremities. Routine labs and physical examination came back normal but a chest x-ray showed possibilities of infection processes, such as inconsistent densities of the lung lining and nodes.
After 8 days in the hospital, the patient’s condition deteriorated, and he began to have a fever in addition to more abnormal growths within the lung. Tests of his sputum indicated Klebsiella pneumonia, Streptococcus pneumonia, and Candida, and the patient was started on antimicrobial and systemic antifungal therapy. On day 18 in the hospital, the patient died.
Post mortem examination had no evidence of carcinomas in the lung, but instead revealed necrotizing Aspergillus pneumonia.
May 1975: Pulmonary Aspergillosis, Inhalation of Contaminated Marijuana Smoke, Chronic Granulomatous Disease by M J Chusid, J A Gelfand, C Nutter, A S Fauci
In this letter published to Annals of Internal Medicine the four authors recount the case of a 17 year old boy with a genetic disease, chronic granulomatous disease (CGD). CGD causes white blood cells to be unable to kill certain bacteria and fungi. Increased susceptibility to infection is expected with such a disease.
Two weeks before hospital admission, the patient noted some ‘malaise’ that set in 12 hours after “smoking several pipefulls of marijuana that had been buried in the earth for ‘aging.’” A few days later, he developed a cough, and night sweats. When he was physically examined at the hospital, it was unremarkable except for an elevated breath rate of 32 respirations per minute (12–18 is normal for an adult). His temperature was slightly elevated at 101 degrees, A chest x-ray did show abnormality, and his blood results showed some signs possible signs of infection / disease (Leukocyte count was 8500/mm3 with 65 % segmented neutrophils, 8% bands, and 5 % eosinophils. Erythrocyte sedimentation rate was 50 mm / min).
Repeated sputum and blood tests came back negative for bacterial and fungal pathogens, and was also negative for tuberculosis. This led to an open thoracotomy, and the biopsy tested positive for A. fumigatus.
The patient received intravenous amphotericin B and prednisolone every 8 hours for the next 5 days, and his partial pressure of oxygen values, which measure the effectiveness of the lungs in transporting oxygen to the blood, improved from a low of 38 returned to a nominal range (normally 75–100 in healthy patients).
Cultures later taken from the cannabis and the pipe the patient used came back positive for various fungi, with heavy growth of A. fumigatus. The authors followed up by testing 10 samples of marijuana from the DEA, and cultures from 2 of the samples grew A. fumigatus. The author’s conclusions were “ The present case shows that marijuana may at times be contaminated with A. fumigatus, and is thus a potential hazard to individuals predisposed to Aspergillus infection. For normal individuals such exposure is probably of little practical significance.”
Other Medical Literature
Case studies isn’t all that the medical literature about aspergillus and cannabis has to offer. Here are some research papers regarding cannabis and aspergillus that do not reference single patients, but instead explore more generalized topics about the risks of aspergillus as it pertains to cannabis.
February 1981 Aspergillus: an inhalable contaminant of marihuana by SL Kagen
In this letter to the editor of the New England Journal of Medicine, Dr Kagen reviews the risks of cannabis use for oncology patients (specifically calling out pediatric oncology). They state, “The medical use of marihuana is not without risks, however, since it may contain such toxic substances as Agent Orange, phencyclidine, and paraquat. Likewise, aspergillus has been cultured from marihuana and was considered the likely source of infection in patients who had invasive pulmonary and allergic bronchopulmonary aspergillosis.”
In addition to culturing 26 marijuana cigarettes, they also used serum samples from 26 marihuana smokers and 10 control subjects who denied using cannabis. 11 of 12 marijuana samples contained aspergillus organisms. 11 of the 21 marijuana smokers, or 52%, had precipitins against aspergillus, as compared to just one of the 10 control subjects. Additionally, Dr. Kagan found that Aspergillus fumigatus spores were easily passed from a lit joint into a specialized air filter.
The doctor concluded their letter by stating it must be assumed that cannabis obtained legally contained pathogenic, inhalable Aspergillus, and that the use of immunosuppressive chemotherapy might put cancer patients at risk.
October 1990: Aspergillosis and marijuana. Annals of Internal Medicine a letter in reaction to Stuart M. Levitz, MD and Richard D. Diamond, MD
This letter was sent in response to this 1990 survey of oncologists that discussed the commonality of oncologists recommending the illegal use of cannabis as an antiemetic (anti-nausea) drug during chemotherapy, and 44% said that they had. Drs Levitz and Diamond wanted to ensure that patients understood the risks of using marijuana. The very first risk that they mention is the prevalence of the presence of Aspergillus species on illicit marijuana — and the fact that immunocompromised patients were at risk (they called infection of immunocompetent patients ‘unlikely’).
May 2006, Pulmonary consequences of marijuana smoking by Andreas Klaus Pfeifer , Peter Lange
The original paper was in Danish, but the English abstract explains that it reviewed several pulmonary risks of smoking cannabis, and Aspergillus is included in the list.
January 2001, with Update in May, 2007: Fungal contamination of tobacco and marijuana (Updated)by P E Verweij, J J Kerremans, A Voss, J F Meis
This letter establishes that “Invasive aspergillosis remains a significant cause of morbidity and mortality in immunocompromised patients, including transplant recipients and those treated for hematological malignancy…However, the risk of invasive aspergillosis associated with tobacco or marijuana smoking is unclear.” The authors, all microbiologists from the Netherlands, examined 98 cigarettes from 14 brands and 7 samples of cannabis.
They created an apparatus to ‘smoke,’ and then measured the amount of four species of aspergillus, whether or not the culture was positive for mold, and penicillium. The results of their tests are below.

Lessons Learned
Immunocompromised is a broader term than many realize — diabetes is a condition which can create an immunosuppressive/ immunocompromised state. Corticosteroids create an immunosuppressive state. COVID-19 as well.
Cannabis use is vastly underreported by patients for the legitimate fear of life-altering prosecution. This is just one part of the reason that there simply isn’t enough research in the intersection of cannabis use and medical issues.
The use of remediation methods, specifically gamma irradiation (as they do in Canada), may not be effective in protecting heavy users.
Aspergillosis is difficult to detect and diagnose even within hospitals, and is often recognized via fungal hyphae found during biopsy or bronchoalveolar lavage.
44% of physicians recommended cannabis use to their cancer patients on chemotherapy to combat nausea. These patients have the immunocompromised status that makes Aspergillus more common. These patients were also key in arguments that lead to the legalization of cannabis for medical use, which paved the way for the adult use market.
Conversations in the cannabis industry about Aspergillus are dominated by IPA, but that is not the only impact of Aspergillus.
There are occupational hazards for cannabis workers such as processors and trimmers, who could be exposed to high-load situations.
Further Reading / Watching
Cannabis Preventive Control w/PhD Micriobiologist Tess Eidem
Pulmonary aspergillosis: a clinical review | European Respiratory Society
Pulmonary consequences of marijuana smoking
A 56-year-old woman with COPD and multiple pulmonary nodules
TOO MANY MOULDY JOINTS — MARIJUANA AND CHRONIC PULMONARY ASPERGILLOSIS
Aspergillosis and marijuana. Annals of Internal Medicine.
Chronic necrotising pulmonary Aspergillosis in a marijuana addict: a new cause of amyloidosis.
Up in smoke: An unusual case of diffuse alveolar hemorrhage from marijuana
Allergic bronchopulmonary aspergillosis associated with smoking moldy marihuana
Aspergillus: an inhalable contaminant of marihuana
Pulmonary aspergillosis, inhalation of contaminated marijuana smoke, chronic granulomatous disease.
Aspergillus nodules; another presentation of Chronic Pulmonary Aspergillosis
Aspergillosis Presenting as Multiple Pulmonary Nodules in an Immunocompetent Cannabis User
Disseminated aspergillosis in an HIV-positive cannabis user taking steroid treatment
Cigarette smoke, bacteria, mold, microbial toxins, and chronic lung inflammation
Cannabis contaminants: sources, distribution, human toxicity and pharmacologic effects
Aspergillus: An Inhalable Contaminant of Marihuana
Marijuana smoking and fungal sensitization
Chronic necrotising pulmonary aspergillosis in a marijuana addict: a new cause of amyloidosis
Pulmonary aspergillosis in the acquired immunodeficiency syndrome
https://www.aspergillus.org.uk/case-histories/
Allergic bronchopulmonary aspergillosis in asthma: epidemiological, clinical and therapeutic issues
Invasive fungal sinusitis in a healthy athlete due to long-term anabolic steroid use
Cigarette smoke, bacteria, mold, microbial toxins, and chronic lung inflammation — interesting but not a case study
Cannabis contaminants: sources, distribution, human toxicity and pharmacologic effects
Marijuana smoking and fungal sensitization
Super interesting read about the rapid, complete recovery from an autism spectrum disorder after treatment of aspergillus with the antifungal drugs itraconazole and sporanox
Chronic pulmonary aspergillosis: rationale and clinical guidelines for diagnosis and management
Invasive aspergillosis in critically ill patients: An autopsy study
Occupational Hazards in Cannabis
Potential exposures associated with indoor marijuana growing operations
Cannabis sativa: the unconventional “weed” allergen
Cannabis contaminants: sources, distribution, human toxicity and pharmacologic effects
Occupational Allergies to Cannabis
An emerging allergen: Cannabis sativa allergy in a climate of recent legalization
Application of the Environmental Relative Moldiness Index in Indoor Marijuana Grow Operations